The Heart
Overview, Position and Coverings
The heart sits in the middle mediastinum inside a tough fibroserous sac — the pericardium — whose outer fibrous layer is so inextensible that even a relatively small accumulation of fluid can fatally compress the ventricles (cardiac tamponade), while the inner serous layer (epicardium) secretes just enough fluid to let the heart glide frictionlessly during its 100,000 daily contractions. The pericardium is innervated entirely by the phrenic nerve (C3–C5), which is why both pericardial and diaphragmatic irritation refer pain to the shoulder tip. On the chest wall, the apex (left 5th ICS midclavicular line) is formed by the LV, and valve sounds are heard downstream from the valve — not directly over it — a principle captured by "All Patients Take Medicine" (Aortic 2R, Pulmonary 2L, Tricuspid 4L, Mitral apex).
The pericardium is a fibroserous sac enclosing the heart and the roots of the great vessels, situated in the middle mediastinum. It consists of an outer fibrous layer and an inner serous layer, and functions to anchor the heart in position while allowing it to contract freely with minimal friction.
When fluid accumulates in the pericardial cavity — from pericarditis (pericardial effusion) or trauma (haemopericardium) — the inextensible fibrous pericardium cannot expand. The mounting pressure compresses the ventricles, impeding filling. This is cardiac tamponade — a medical emergency. Classic signs: distended neck veins, muffled heart sounds, falling pulse pressure (Beck's Triad). Emergency treatment: pericardiocentesis — needle inserted into the 5th/6th intercostal space adjacent to the sternum, exploiting the cardiac notch in the left lung. [Netter's 5th §22 p158]
Cardiac Tamponade: Acute (trauma, aortic dissection, malignant effusion, uraemia, post-MI Dressler's). Pathology: fluid in pericardial space compresses all four chambers throughout the cardiac cycle.
Signs: Beck's Triad (↑JVP + muffled heart sounds + hypotension); pulsus paradoxus >10 mmHg (exaggerated fall in systolic BP with inspiration — because inspiration → RV fills more → septum shifts left → less LV filling → ↓ systolic BP); tachycardia; no Kussmaul's sign (JVP FALLS on inspiration = normal — because pericardial fluid is pliable and accommodates increased RV filling). ECG: low-voltage complexes, electrical alternans (swinging heart). Echo: RA/RV diastolic collapse = diagnostic. Treatment: pericardiocentesis (emergency drain).
Constrictive Pericarditis: Chronic (prior TB = most common globally; prior cardiac surgery; prior radiation therapy; viral/idiopathic). Pathology: fibrous/calcified rigid pericardial shell encases the heart — fixed end-diastolic volume, equal filling pressures all four chambers (ventricular interdependence).
Signs: ↑JVP with prominent x + y descents; Kussmaul's sign (JVP RISES on inspiration — normal negative intrathoracic pressure cannot be transmitted through rigid pericardium → blood has nowhere to go → JVP rises); no pulsus paradoxus; pericardial knock (early S3 equivalent, high frequency, early diastole); hepatomegaly + ascites + lower limb oedema (chronic venous hypertension). CXR: pericardial calcification (seen in 50% of TB constrictive); CT/MRI: pericardial thickening >4 mm. Echo: respiratory variation in E-wave flow velocities >25% (tissue Doppler + hepatic vein flow reversal). Equalisation of end-diastolic pressures (RVEDP = LVEDP ± 5 mmHg) on cardiac catheterisation = gold standard. Treatment: pericardiectomy (surgical stripping) = definitive; diuretics for symptoms.
Key distinguishing features:
Pulsus paradoxus → Tamponade (not constrictive)
Kussmaul's sign → Constrictive (not tamponade)
Pericardial knock → Constrictive
Pericardial calcification → Constrictive
Electrical alternans → Tamponade
Left border — formed mainly by the left ventricle; from the 2nd left intercostal space to the apex.
Superior border — level of the 2nd costal cartilages bilaterally; great vessels emerge here.
Inferior border — from the 6th right costal cartilage to the apex.
Apex — left 5th intercostal space, midclavicular line (~9 cm from midline); formed by the left ventricle; the site of the apex beat (point of maximum impulse).
PV2L — Pulmonary valve heard over 2nd Left intercostal space
AV2R — Aortic valve heard over 2nd Right intercostal space
Tricuspid — lower left sternal edge (4th ICS) | Mitral — Apex (5th ICS MCL)
Tip: "All Patients Take Medicine" — Aortic, Pulmonary, Tricuspid, Mitral (right→left, top→bottom)
- Beck's Triad in cardiac tamponade? ↑JVP (distended neck veins) + muffled heart sounds + hypotension. Treatment = emergency pericardiocentesis. ECG: low-voltage + electrical alternans
- Tamponade vs constrictive pericarditis — one key difference each? Tamponade: pulsus paradoxus >10 mmHg; NO Kussmaul's sign. Constrictive: Kussmaul's sign (JVP rises on inspiration); NO pulsus paradoxus; pericardial knock; pericardial calcification on CXR
- Why does pericardial pain refer to the shoulder tip? Phrenic nerve (C3–C5) innervates the pericardium; the same dermatomal segments supply the shoulder skin → referred pain to shoulder tip
- Heart apex: location and which chamber? Left 5th intercostal space, midclavicular line (~9 cm from midline); formed entirely by the left ventricle
- "All Patients Take Medicine" — what does it tell you? Auscultation areas from upper right to apex: Aortic 2nd right ICS; Pulmonary 2nd left ICS; Tricuspid 4th left sternal edge; Mitral apex (5th ICS MCL)
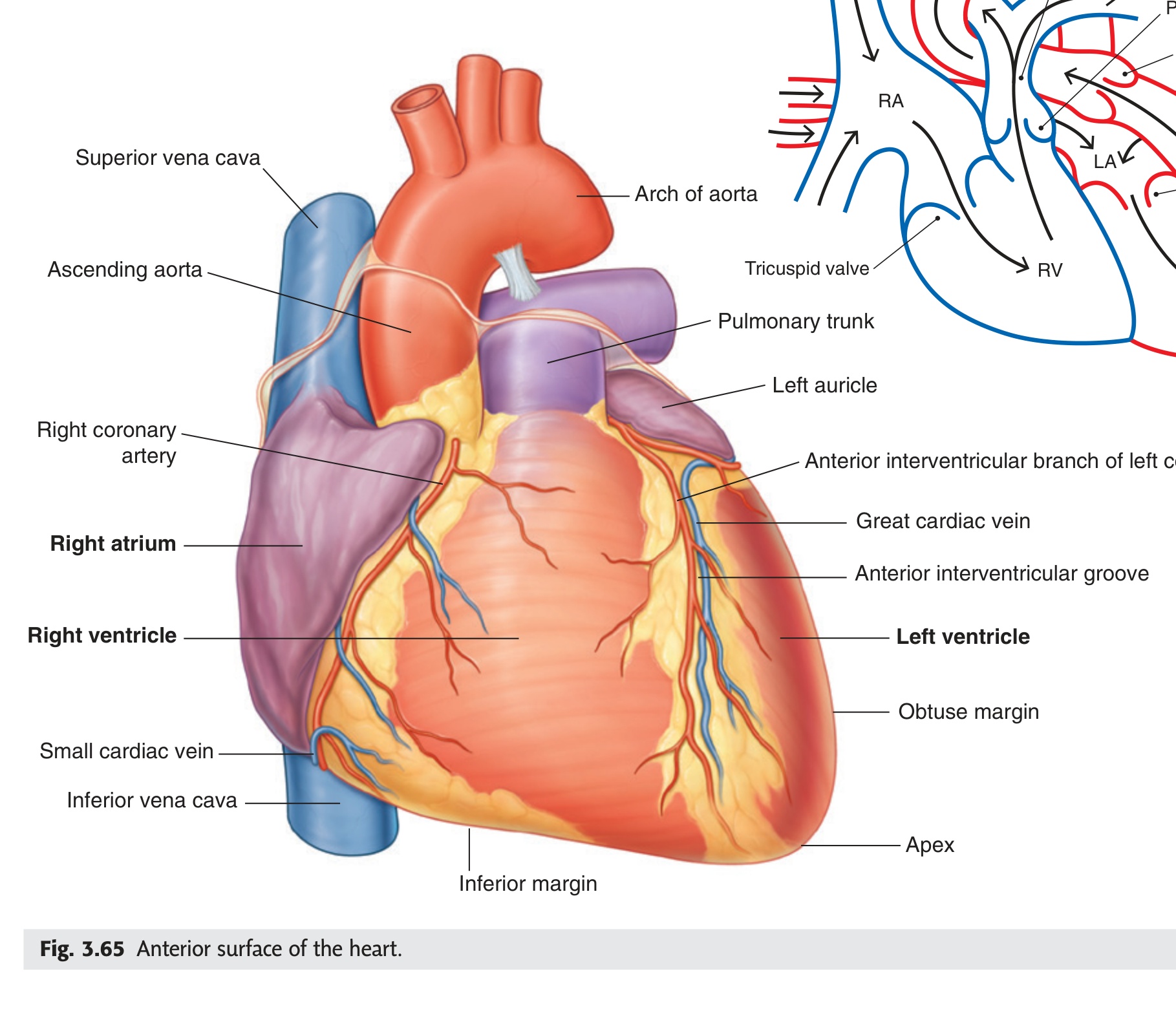
Internal Features of the Cardiac Chambers
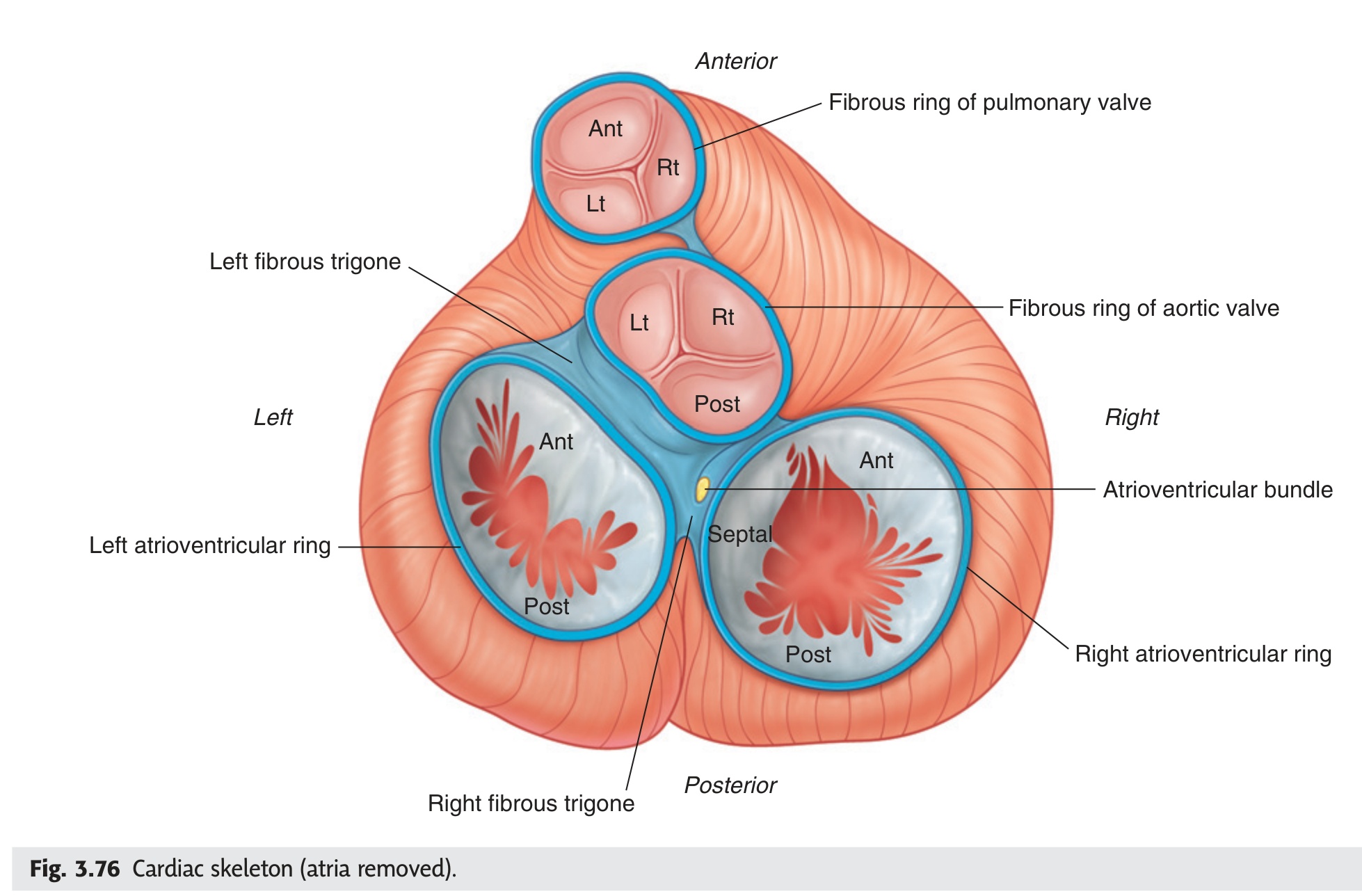
All four cardiac chambers share one organising principle: smooth walls for outflow, rough trabeculae carneae for inflow, with papillary muscles and chordae tendineae tethering the AV valve cusps so that rising ventricular pressure closes the valve while simultaneously preventing it from prolapsing into the atrium. The LV wall is three times thicker than the RV because it pumps against systemic resistance (~120 mmHg) rather than the low-pressure pulmonary circuit (~25 mmHg), and this asymmetry explains the ECG dominance pattern and the different consequences of failure in each. The cardiac fibrous skeleton (four fibrous rings + right and left trigones) anchors all four valves, electrically isolates atria from ventricles, and is pierced at the right fibrous trigone by the AV bundle (Bundle of His) as the sole conducting pathway between the chambers.
The right atrium is the thin-walled, posterosuperior chamber of the right heart, receiving deoxygenated blood from the systemic venous circulation and delivering it to the right ventricle via the right atrioventricular orifice.
- Orifice of the superior vena cava — returns deoxygenated blood from the upper half of the body (head, neck, upper limbs)
- Orifice of the inferior vena cava — returns deoxygenated blood from the lower half of the body (trunk, lower limbs, abdominal viscera)
- Orifice of the coronary sinus — returns venous blood from the myocardium (cardiac muscle) itself
The fossa ovalis is the commonest site of atrial septal defect (ASD). A patent foramen ovale (PFO) persists in ~25–30% of adults and can allow paradoxical emboli (venous clots crossing to the arterial circulation), causing cryptogenic stroke.
The right ventricle is the anterosuperior chamber of the right heart, receiving deoxygenated blood from the right atrium and pumping it through the pulmonary orifice into the pulmonary trunk for oxygenation in the lungs.
Outflowing part (conus arteriosus / infundibulum): smooth-walled, cone-shaped, directs blood upward to the pulmonary orifice, guarded by the pulmonary valve (3 semilunar cusps: anterior, right, left).
The tricuspid complex is the collective term for the four structural components that together prevent backflow of blood from the right ventricle into the right atrium during ventricular systole.
- Right atrioventricular fibrous ring — the annular fibrous skeleton anchoring the valve cusps.
- Tricuspid valve cusps — three cusps (anterior, posterior, septal) projecting into the ventricular lumen. Their free edges face downward into the ventricle.
- Chordae tendineae — strong tendinous cords attaching the free edges and ventricular surfaces of the cusps to the papillary muscles. They prevent the cusps from inverting into the atrium during systole.
- Papillary muscles — three cone-shaped muscular projections (anterior, posterior, septal) arising from the ventricular wall. They contract simultaneously with the ventricle, maintaining chordae tension throughout systole.
When the tricuspid complex fails — from right ventricular dilation stretching the annulus, or rheumatic disease — blood leaks back into the right atrium during systole. This raises right atrial and venous pressure, causing: raised jugular venous pressure (JVP), peripheral oedema, hepatomegaly, and ascites — the classic signs of right heart failure.
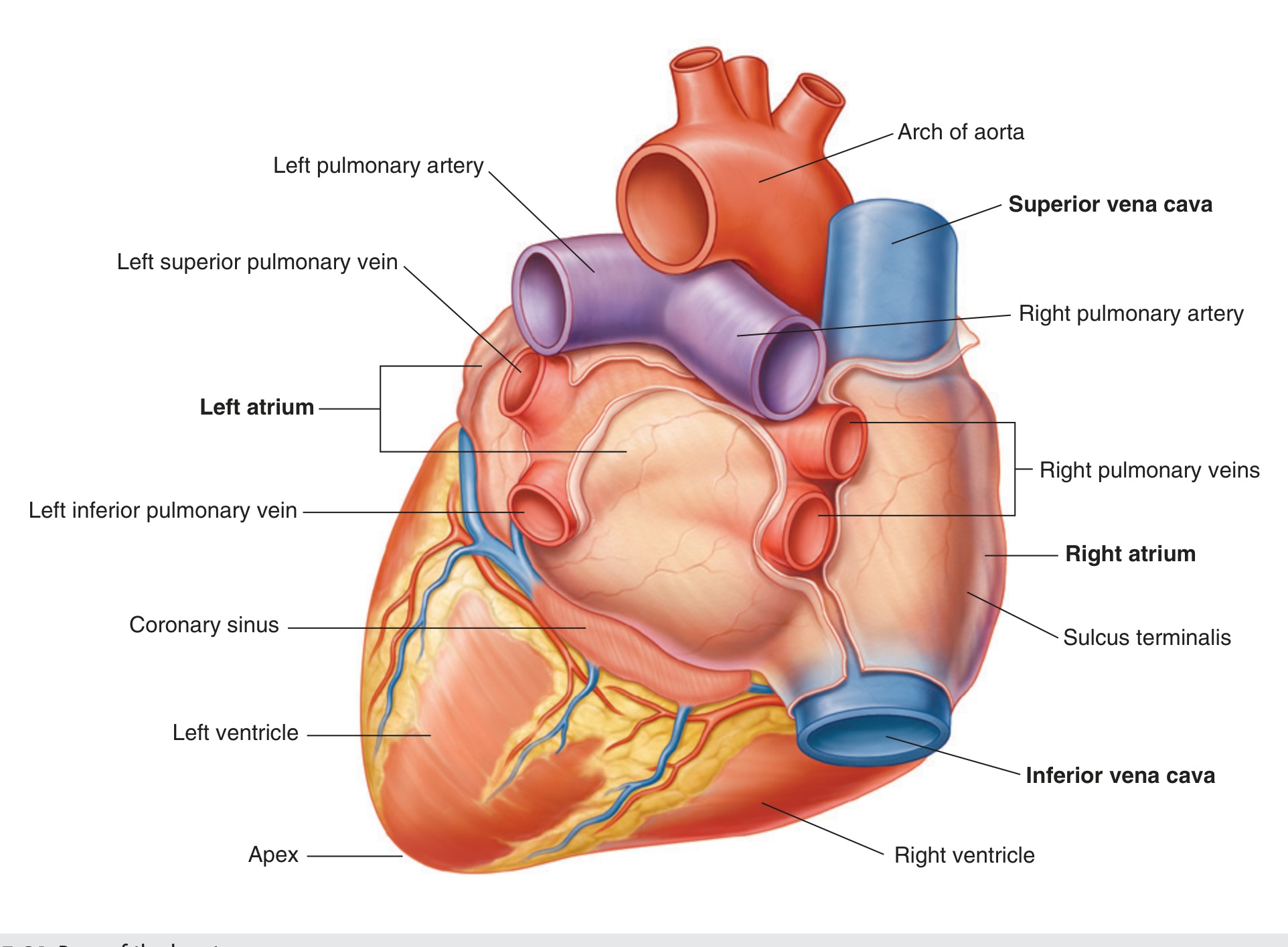
The left atrium is the posterosuperior chamber of the left heart, receiving oxygenated blood from the four pulmonary veins and delivering it to the left ventricle via the left atrioventricular orifice.
One outlet: the left atrioventricular orifice — guarded by the bicuspid (mitral) valve; leads blood into the left ventricle.
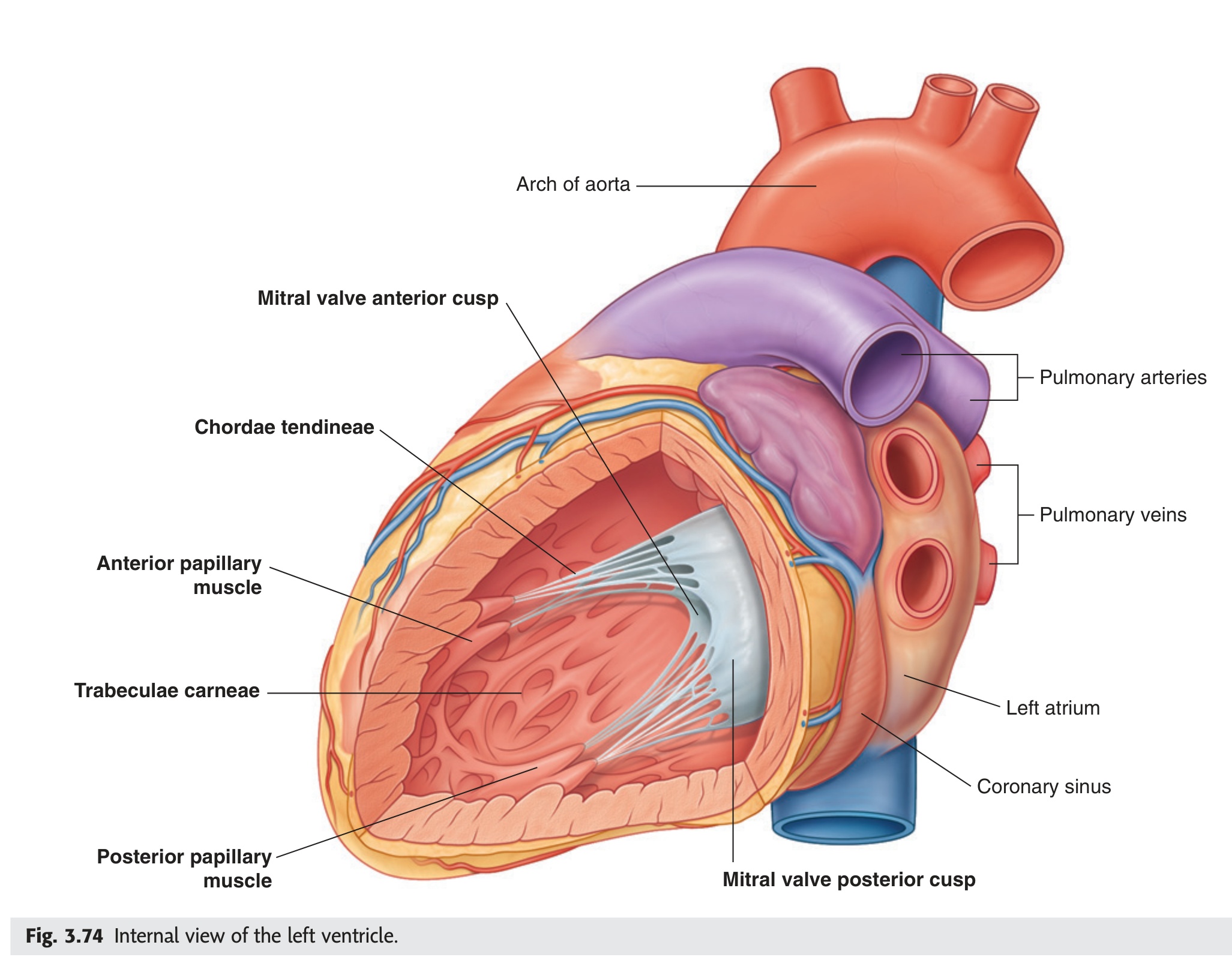
The left ventricle is the posteroinferior chamber of the left heart that receives oxygenated blood from the left atrium and pumps it into the aorta for systemic distribution. Its wall is approximately three times as thick as the right ventricle, reflecting the much higher pressures it must generate.
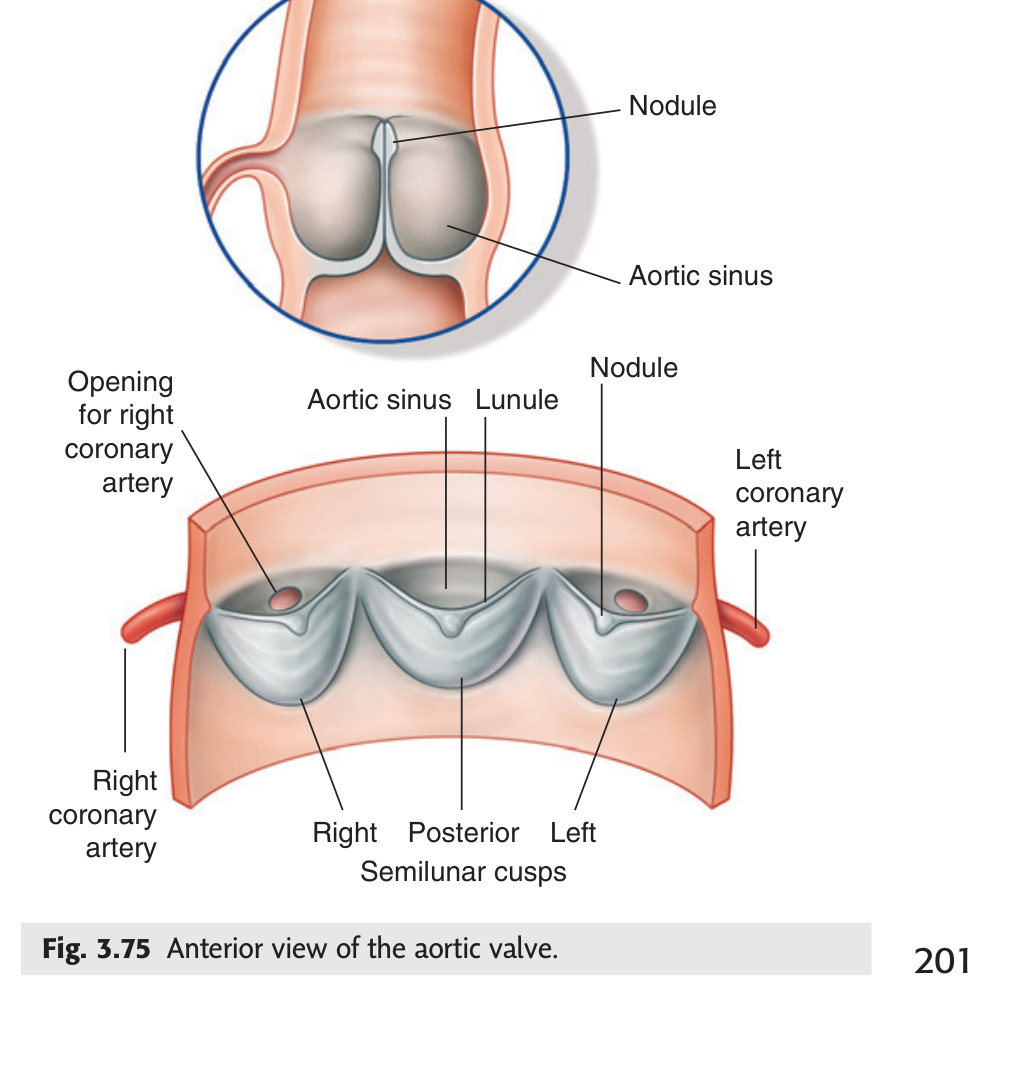
Outflowing part (aortic vestibule): smooth-walled. Leads to the aortic orifice guarded by the aortic valve (three semilunar cusps: posterior, right, left). Above the aortic valve cusps, the aortic wall bulges outward to form the aortic sinuses (sinuses of Valsalva) — the right and left aortic sinuses give rise to the right and left coronary arteries respectively.
The bicuspid complex is the set of four structural components guarding the left atrioventricular orifice that together prevent backflow of blood from the left ventricle into the left atrium during ventricular systole.
- Left atrioventricular fibrous ring — the structural anchor for the bicuspid valve cusps.
- Bicuspid valve cusps — two cusps (anterior and posterior). The mitral valve is the most frequently diseased heart valve.
- Chordae tendineae — tether the free edges of the cusps to the papillary muscles below, preventing inversion into the left atrium.
- Papillary muscles — anterior and posterior; contract simultaneously with the left ventricle to maintain chordae tension throughout systole.
The mitral valve is the most frequently diseased heart valve — particularly in rheumatic heart disease and infective endocarditis. Mitral regurgitation allows backflow into the left atrium, producing a high-pitched pansystolic murmur loudest at the apex. Longstanding mitral regurgitation leads to left atrial enlargement, pulmonary hypertension, and eventually left ventricular failure. [Netter's 5th §22 p172]
- Three inlets of the right atrium? Superior vena cava (upper body), inferior vena cava (lower body), coronary sinus (myocardium). One outlet = right AV orifice (tricuspid valve)
- What is the moderator band (septomarginal trabecula) and why does it matter? Muscular band crossing RV from IVS to anterior papillary muscle; carries right bundle branch of AV bundle → mechanical trauma to RV can cause RBBB
- Four components of the tricuspid complex? (1) Right AV fibrous ring; (2) three cusps (anterior, posterior, septal); (3) chordae tendineae; (4) papillary muscles — all prevent RV-to-RA backflow during systole
- Why is the LV wall 3× thicker than the RV? LV pumps against systemic resistance (~120 mmHg); RV pumps against pulmonary resistance (~25 mmHg) — wall thickness reflects workload
- Which aortic sinus gives rise to the RCA and which to the LCA? RCA from right (anterior) aortic sinus; LCA from left aortic sinus; posterior (non-coronary) sinus faces interatrial septum — no coronary artery
Conduction System of the Heart ★★★
The heart's electrical system is a hierarchy of failsafe pacemakers: the SA node fires at 60–100/min and is the default initiator; if it fails, the AV node takes over at 40–60/min; if that fails, Purkinje fibres fire at 30–40/min — a rate that sustains life but causes haemodynamic compromise requiring an implanted pacemaker. The AV node is not merely a relay — its 0.1-second delay is a precision timing device that allows atrial contraction to complete and the ventricles to fill before ventricular systole begins, maximising stroke volume. The right bundle branch runs physically inside the moderator band, which is why blunt chest trauma to the RV can cause RBBB — the conducting tissue is mechanically disrupted by that specific anatomical arrangement.
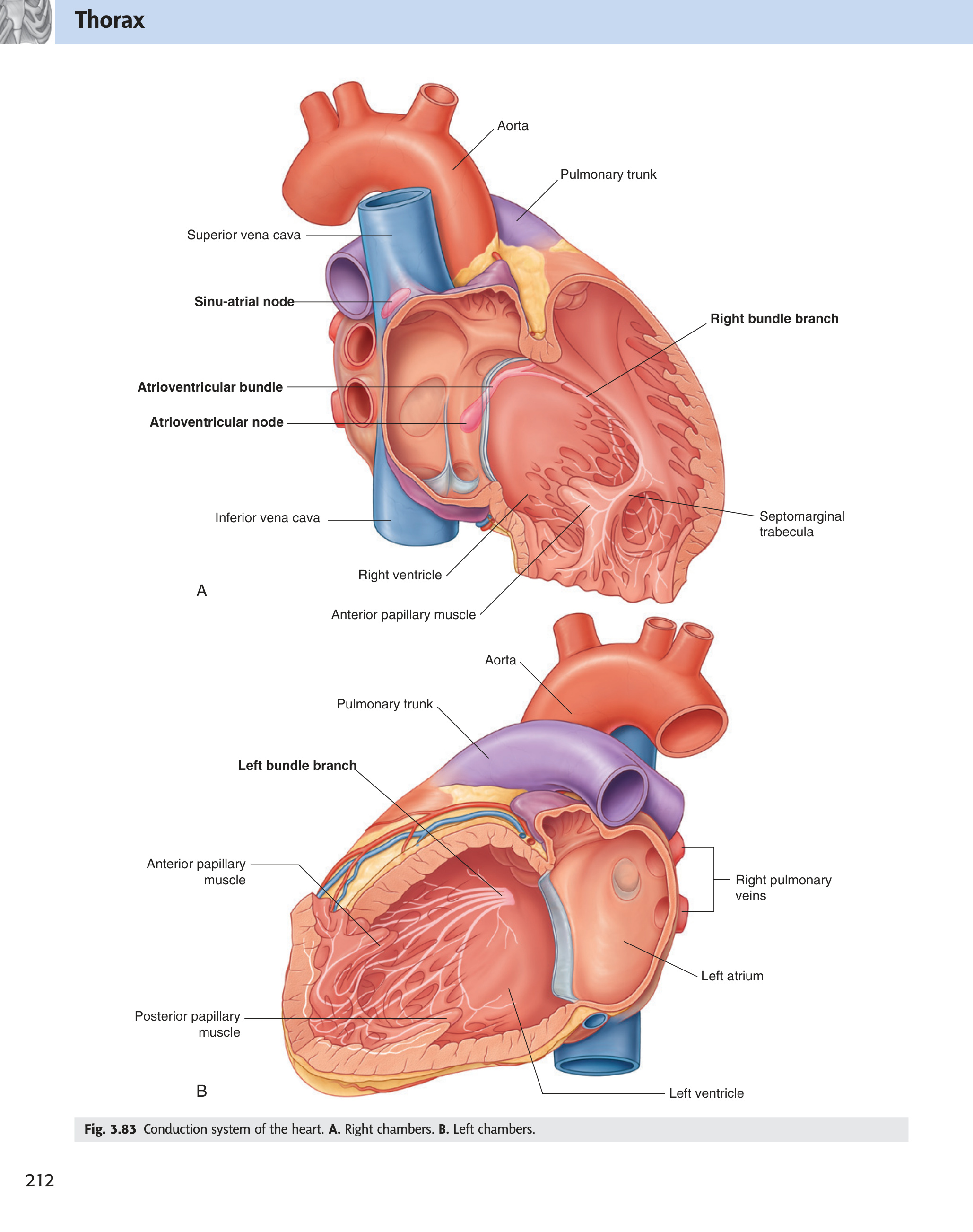
The cardiac conduction system is a network of specialised myocardial fibres that spontaneously generates and coordinates electrical impulses, ensuring the sequential, rhythmic contraction of the atria followed by the ventricles at an appropriate rate.
- Sinoatrial node (SA node) — in the wall of the right atrium, near the opening of the superior vena cava. The pacemaker of the heart — spontaneously depolarises at 60–100/min, initiating each cardiac cycle.
- Internodal tracts — three pathways (anterior, middle, posterior) conducting the impulse through the atrial walls to the AV node, causing atrial contraction en route.
- Atrioventricular node (AV node) — in the interatrial septum near the opening of the coronary sinus. Introduces a brief delay (~0.1 seconds) — allowing atrial contraction to complete and ventricular filling to occur before ventricular systole begins.
- Atrioventricular bundle (Bundle of His) with right and left bundle branches — passes from the AV node into the interventricular septum; the right bundle branch runs within the septomarginal trabecula (moderator band) to the right ventricular wall; the left bundle branch passes through the septum to the left ventricular wall.
- Subendocardial plexus of Purkinje fibres — terminal network of large, rapidly-conducting fibres spreading from the bundle branches throughout both ventricular walls. Their rapid conduction ensures near-simultaneous ventricular depolarisation, producing a single powerful coordinated contraction. [Gray's 4e Ch3 p188]
SA node (60–100/min) → AV node (40–60/min) → Purkinje fibres (30–40/min)
Each level becomes the pacemaker if the one above it fails. At Purkinje rate (30–40/min) the patient is haemodynamically compromised → requires an implanted cardiac pacemaker.
- Failsafe pacemaker hierarchy with rates? SA node 60–100/min → AV node 40–60/min → Purkinje fibres 30–40/min. Each takes over if the level above fails; Purkinje rate = haemodynamically compromised → needs implanted pacemaker
- Five components of the conduction system in order? SA node → internodal tracts → AV node → AV bundle (Bundle of His) + right/left bundle branches → subendocardial Purkinje fibre plexus
- Where does the right bundle branch run and clinical significance? Inside the septomarginal trabecula (moderator band) across the RV; blunt chest trauma can cause RBBB by physically disrupting it
- SA node location and blood supply? Wall of right atrium near SVC orifice; supplied by SA nodal artery (branch of RCA 60%, LCA circumflex 40%)
- AV node location and blood supply? Interatrial septum near coronary sinus orifice; supplied by AV nodal artery (RCA in 80–90%) — explains why inferior MI (RCA) causes AV block
Coronary Circulation ★★★
The coronary arteries are unique in receiving blood primarily during diastole — not systole — because systolic ventricular contraction compresses the intramural vessels; this is why tachycardia (shortened diastole) paradoxically starves the working heart of oxygen at exactly the moment it needs it most. The LAD ("widow maker") supplies the largest territory — anterior LV, anterior two-thirds of the IVS, and both bundle branches — so a proximal LAD occlusion simultaneously kills myocardium, disrupts conduction (LBBB or complete AV block), and causes cardiogenic shock. The RCA supplies the inferior wall, the right ventricle, and in 80–90% of people the AV node — so inferior STEMI (ST↑ II, III, aVF) is almost always an RCA occlusion, and any associated AV block is from nodal ischaemia; critically, RV infarction in this setting makes nitrates lethal by collapsing preload.
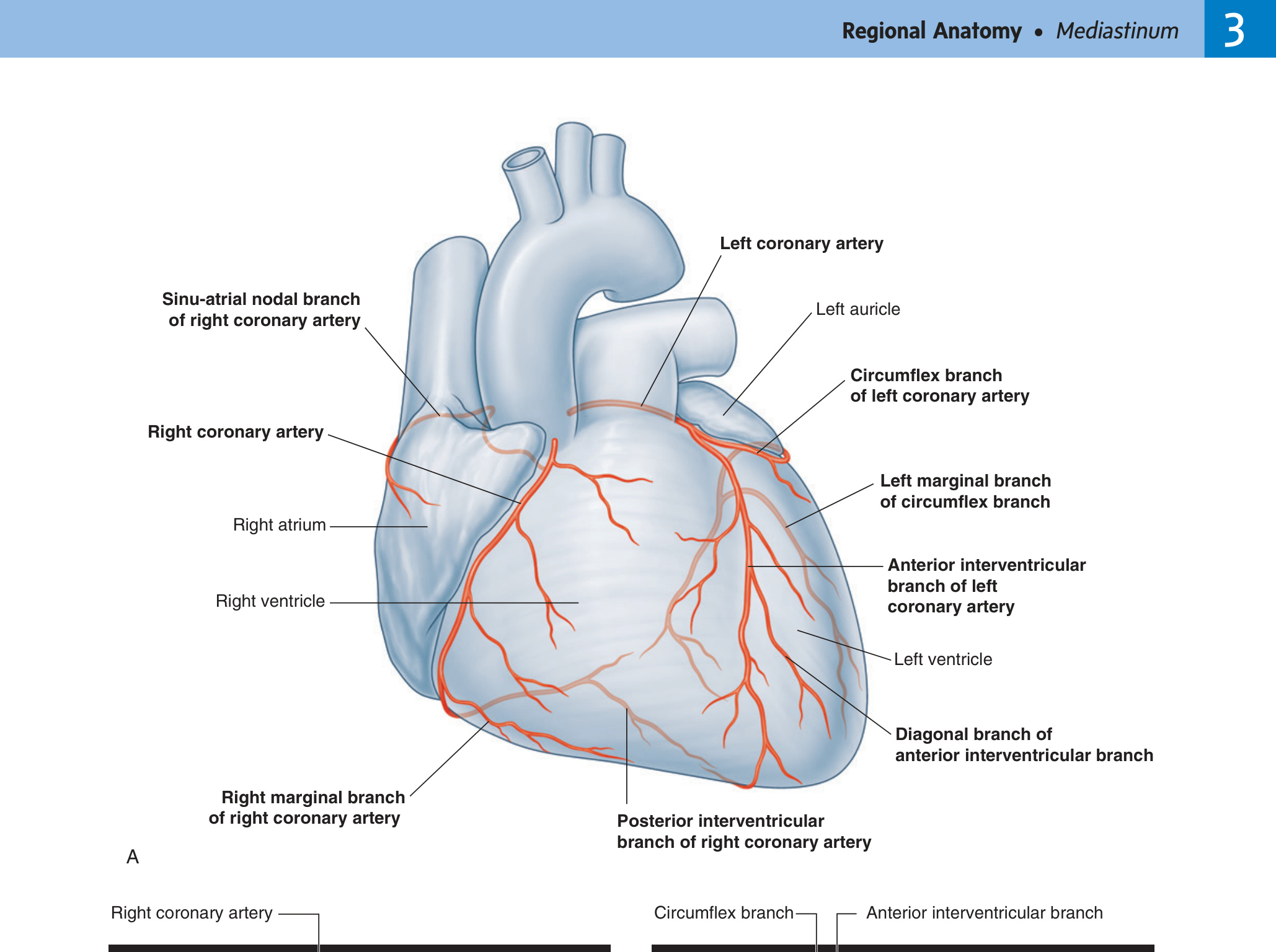
The coronary arteries are the first branches of the aorta, arising from the aortic sinuses (sinuses of Valsalva) immediately above the aortic valve cusps, and supplying the entire myocardium with oxygenated blood.
| Vessel | Origin | Main Branches | Territory Supplied |
|---|---|---|---|
| Right Coronary Artery (RCA) | Right aortic sinus | Posterior interventricular branch (posterior descending artery); Posterior branch of left ventricle; SA nodal branch; AV nodal branch | Right atrium, right ventricle, posterior septum, posterior left ventricle, SA node (60%), AV node (80–90%) |
| Left Coronary Artery (LCA) | Left aortic sinus | Anterior interventricular branch (LAD); Circumflex branch | Anterior walls of both ventricles, anterior 2/3 of interventricular septum (LAD); left atrium, posterior left ventricle (circumflex) |
The left anterior descending artery (LAD) — the "widow maker" — supplies the largest amount of ventricular muscle. Its occlusion causes a large anterior myocardial infarction with high mortality. In CABG surgery, the internal thoracic artery or saphenous vein is grafted to bypass the occlusion, restoring distal perfusion. [Netter's 5th §22 p158]
Cardiac ischaemic pain is referred to the left pectoral region and medial left arm because visceral afferent fibres from the heart enter spinal cord segments T1–T4/T5 on the left — the same segments receiving somatic sensory input from the chest wall and arm. The brain misinterprets the cardiac signal as coming from the arm.
The myocardium is drained by two routes: (1) the coronary sinus — the main channel collecting ~65% of cardiac venous return — and (2) direct drainage into the right atrium via the anterior cardiac veins and Thebesian veins.
| Vein | Course | Territory Drained |
|---|---|---|
| Great cardiac vein | Ascends alongside the LAD in the anterior IV groove → turns left alongside the circumflex in the left AV groove → enters left end of coronary sinus | Anterior LV, anterior IVS, both ventricles anteriorly |
| Middle cardiac vein | Ascends alongside the posterior IV artery (PDA) in the posterior IV groove → enters right end of coronary sinus | Posterior LV, posterior IVS |
| Small cardiac vein | Runs alongside the RCA in the right AV groove → enters right end of coronary sinus (or directly into RA) | Posterior right atrium and right ventricle |
| Posterior vein of LV | Runs on the posterior LV surface → enters coronary sinus | Posterior left ventricle |
| Oblique vein of LA (vein of Marshall) | Descends on posterior LA → joins great cardiac vein | Vestige of left SVC; small LA drainage |
Cardiac Resynchronisation Therapy (CRT): In heart failure with bundle branch block, a biventricular pacemaker is implanted. The LV lead is placed via femoral vein → IVC → right atrium → coronary sinus → left lateral vein to pace the lateral LV wall, resynchronising LV contraction. Fluoroscopic knowledge of coronary sinus anatomy is essential for EP cardiologists.
Retrograde cardioplegia: During open-heart surgery, cardioplegia solution is infused via a cannula in the coronary sinus and travels retrogradely through the cardiac veins to achieve uniform myocardial cooling and arrest — useful when antegrade (aortic root) delivery is inadequate (e.g. severe aortic regurgitation). [Gray's 4e Ch3 p209]
Each coronary artery supplies a defined territory. Occlusion causes infarction of that territory, reflected in ECG changes in specific leads. Knowing artery → territory → ECG leads → complications is high-yield for both written and clinical exams.
| Artery Occluded | Territory Infarcted | ECG Leads (ST↑/Q waves) | Key Complications |
|---|---|---|---|
| LAD (left anterior descending) | Anterior LV wall, anterior 2/3 of IVS, RV anterior wall (if proximal), apex, bundle branches | V1–V4 (anterior MI) | LV failure, LBBB, complete heart block (proximal LAD), VSD (septal perforation), cardiogenic shock — highest mortality |
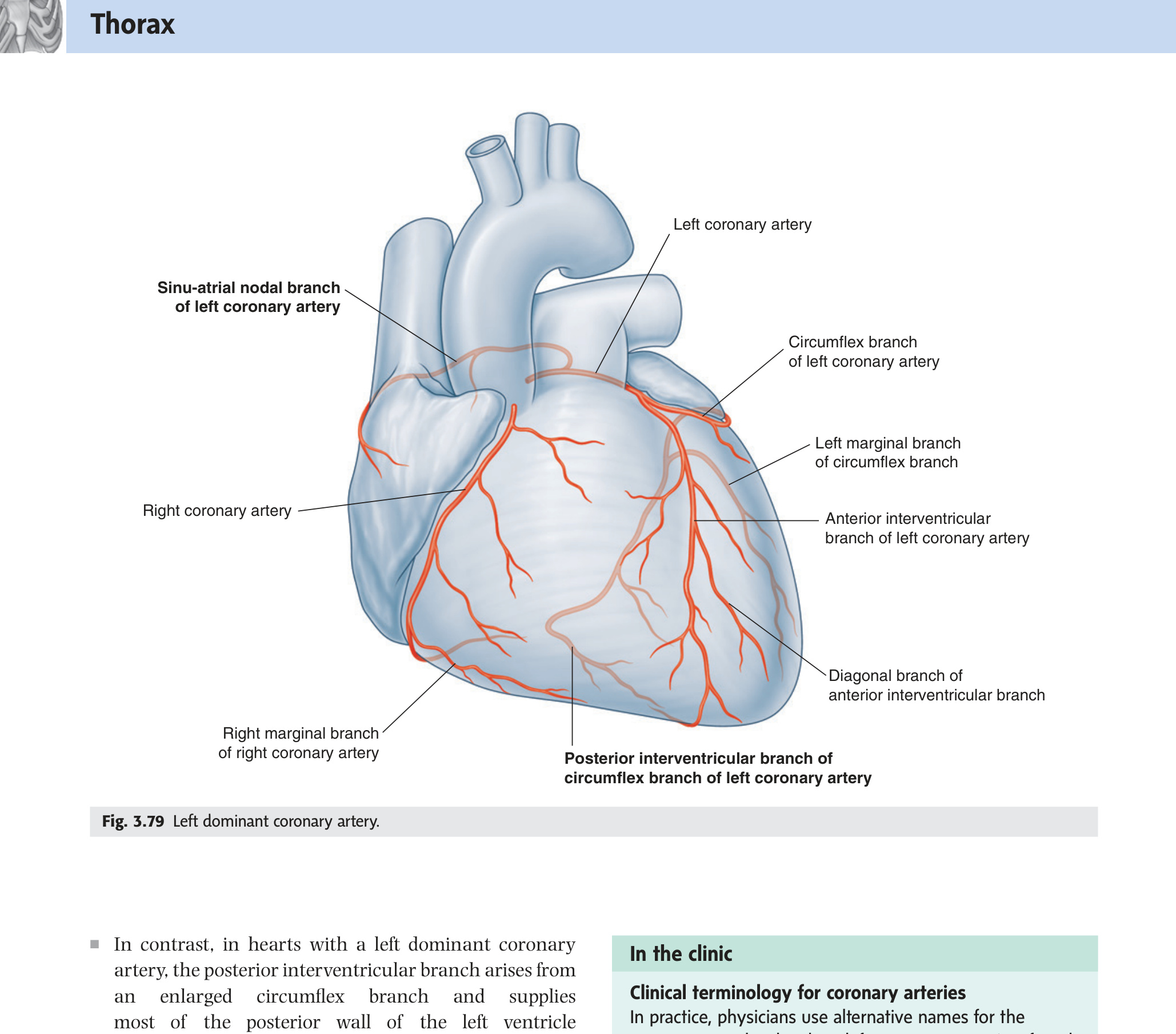
| Circumflex (CX) | Lateral LV wall; posterior LV + posterior IVS if left-dominant | I, aVL, V5–V6 (lateral MI); posterior MI if dominant: tall R V1–V2 + ST↓ | Mitral regurgitation (posterior papillary muscle); generally smaller infarct; may be silent |
| RCA (right coronary artery) | Inferior LV + posterior LV, inferior IVS, RV (RV infarction in 30–40%), SA node (60%), AV node (80–90%) | II, III, aVF (inferior MI); ST↑ V3R–V4R if RV infarction | AV block (1st–3rd degree), sinus bradycardia, RV infarction, posterior papillary muscle rupture → acute MR, Bezold-Jarisch reflex |
LAD = "Widow Maker": largest myocardial territory; proximal LAD occlusion → massive anterior MI + cardiogenic shock.
Inferior MI + RV infarction: In 30–40% of RCA occlusions, the RV is also infarcted. Presents with raised JVP, hypotension, clear lung fields (not pulmonary oedema) and Kussmaul's sign. Critical: AVOID nitrates — they reduce venous return (preload) and will precipitate cardiovascular collapse. Treat with IV fluids to maintain RV filling pressure.
Posterior papillary muscle vulnerability: The posterior papillary muscle (PPM) has a single blood supply from the RCA and is therefore MORE vulnerable to ischaemia than the anterior papillary muscle (dual supply from LAD + circumflex). PPM rupture causes acute severe mitral regurgitation — a catastrophic complication of inferior MI.
Bezold-Jarisch reflex: Inferior MI activates vagal afferents in the inferior LV wall → reflex bradycardia + hypotension + nausea — the classic "vagotonic inferior MI" presentation.
Right coronary dominance (85% of population): RCA gives the PDA and AV nodal artery → RCA occlusion causes inferior MI AND is responsible for most AV block complicating inferior MI. [Gray's 4e Ch3 p200; Gray's 4e p202 — coronary dominance]
- Why does tachycardia worsen myocardial ischaemia? Coronary flow occurs mainly in diastole (systolic contraction compresses intramural vessels); tachycardia shortens diastole → reduced coronary perfusion time → ischaemia in stenosed vessels
- LAD occlusion: territory, ECG leads, key complications? Anterior LV + anterior 2/3 IVS + bundle branches; ST↑ V1–V4; complications: LV failure, LBBB, complete heart block (proximal), VSD, cardiogenic shock — highest mortality
- RCA occlusion: territory, ECG leads, key complications? Inferior LV + posterior LV + RV + SA/AV nodes; ST↑ II, III, aVF; complications: AV block (1st–3rd degree), sinus bradycardia, RV infarction (ST↑ V3R–V4R)
- Why is nitrate contraindicated in RV infarction? RV infarction = preload-dependent LV filling; nitrates → venodilation → ↓ venous return → cardiovascular collapse. Give IV 0.9% NaCl instead
- Where does the coronary sinus lie and where does it drain? Posterior AV (coronary) groove; drains into right atrium between IVC orifice and tricuspid orifice, guarded by the valve of the coronary sinus (Thebesian valve)
Aortic & Pulmonary Valves ★★
The aortic valve's three semilunar cusps each face a sinus of Valsalva: the right and left sinuses give rise to the RCA and LCA respectively, while the posterior (non-coronary) sinus faces the interatrial septum. These sinuses prevent the open cusps from occluding the coronary ostia during systole and generate vortices that efficiently swing the cusps closed in diastole — a design that a bicuspid aortic valve (1–2% of population, most common congenital cardiac anomaly) disrupts, causing calcification and stenosis a full decade earlier than a normal tricuspid valve. Cardiac pain is referred to the left arm because visceral afferent fibres from ischaemic myocardium enter the spinal cord at T1–T4 on the left — the same dermatomes that supply the chest wall and medial arm — so the brain attributes the cardiac signal to its more familiar somatic territory.
| Cusp | Name | Coronary Artery Origin |
|---|---|---|
| Right (anterior) | Right coronary cusp | Right coronary artery (RCA) arises from right aortic sinus |
| Left (posterior-left) | Left coronary cusp | Left coronary artery (LCA) arises from left aortic sinus |
| Posterior (non-facing) | Non-coronary (posterior) cusp | No coronary artery — faces interatrial septum |
Sinuses of Valsalva (aortic sinuses): Small bulbous dilatations of the aortic root behind each cusp. They prevent cusps from occluding coronary ostia during systolic opening, and generate vortices that help cusps close efficiently in early diastole. The aortic root is supported by the fibrous skeleton of the heart (annulus fibrosus). Sinus of Valsalva aneurysm: rare; right sinus most common; can rupture into RV → continuous murmur + acute decompensation.
Aortic stenosis triad (SAD = progressive severity/prognosis): Syncope → Angina → Dyspnoea (heart failure). Average survival after symptoms: syncope = 3 years; angina = 5 years; dyspnoea = <2 years without intervention. Signs: slow-rising (pulsus parvus et tardus) carotid pulse; narrow pulse pressure; ejection systolic murmur radiating to carotids; paradoxical split S2. Severe = valve area <1 cm², mean gradient >40 mmHg. Treatment: surgical AVR or TAVI (transcatheter aortic valve implantation — via femoral artery).
Pulmonary valve: 3 semilunar cusps (anterior, left, right). No coronary orifices behind the pulmonary sinuses. Isolated valvular pulmonary stenosis = balloon valvuloplasty. Pulmonary regurgitation is well tolerated for years; most commonly iatrogenic (after ToF repair).
| Nerve Supply | Source | Effect |
|---|---|---|
| Sympathetic (accelerator) | Cardiac branches of stellate ganglion (T1–T4/5); reach heart via cardiac plexus | ↑ heart rate (chronotropy), ↑ force (inotropy), ↑ conduction velocity; coronary vasodilation (β₂); pain fibres travel with sympathetics (T1–T4 → referred angina to left chest/arm) |
| Parasympathetic (vagal) | Cardiac branches of vagus (CN X); superficial + deep cardiac plexus at base of heart | ↓ heart rate (SA node), ↓ AV conduction (PR prolongation); minimal effect on ventricular contractility; carotid sinus massage/Valsalva → ↑ vagal tone → slows SVT |
| Cardiac plexus | Superficial (below aortic arch) + deep (between aortic arch + tracheal bifurcation) | Both sympathetic + parasympathetic fibres reach SA node, AV node, coronary arteries via plexus; sensory fibres accompany sympathetics back to spinal cord |
Visceral afferent fibres from ischaemic myocardium travel with sympathetic fibres → enter spinal cord at T1–T4 (predominantly left). These same segments receive somatic input from the left chest wall, shoulder, medial arm, and jaw. The brain misinterprets the cardiac signal as coming from these somatic regions → referred pain to left pectoral area + medial left arm + jaw. Right-sided ischaemia (RCA territory) can occasionally refer to the right arm. Inferior MI (RCA) often presents with epigastric pain (T5 referral via diaphragmatic irritation).
- Which aortic sinuses give rise to coronary arteries, and what does the third face? Right sinus → RCA; left sinus → LCA; posterior (non-coronary) sinus faces interatrial septum — no coronary artery
- Bicuspid aortic valve: prevalence, most common complication, associated lesion? 1–2% of population (M:F 3:1); most common = aortic stenosis (calcifies decade earlier than tricuspid valve); associated with coarctation of aorta (50% of coarctation patients have BAV)
- Aortic stenosis triad (SAD) with survival after each symptom? Syncope (~3 years), Angina (~5 years), Dyspnoea/heart failure (<2 years) — prognosis worsens progressively; treat with AVR or TAVI
- Why does cardiac ischaemic pain refer to the left arm? Visceral afferents travel with sympathetics → enter cord at T1–T4 left; same segments receive somatic input from left chest wall + medial arm → brain attributes pain to somatic territory
- Carotid sinus massage treats which arrhythmias and how? SVT (supraventricular tachycardias); increases vagal tone → slows AV conduction → terminates re-entrant circuits through the AV node (AVNRT, AVRT)
Congenital Heart Disease ★★★
Congenital heart disease splits cleanly into lesions that are pink at birth (acyanotic, left-to-right shunts overloading the pulmonary circulation) and those that are blue at birth (cyanotic, right-to-left shunts bypassing the lungs entirely). Left-to-right shunts (VSD, ASD, PDA) are silent early but if unrepaired cause pulmonary hypertension that eventually reverses the shunt — Eisenmenger syndrome, an irreversible cyanotic state. Tetralogy of Fallot, the most common cyanotic CHD, is anatomically a single embryological error — anterior deviation of the infundibular septum — that simultaneously creates a large VSD, obstructs the right ventricular outflow, forces the aorta to override the VSD, and hypertrophies the RV in response; cyanosis severity tracks outflow obstruction severity, not the VSD size.
| Lesion | Frequency | Anatomy & Pathophysiology | Key Signs & Treatment |
|---|---|---|---|
| VSD (ventricular septal defect) | Most common CHD (30%) | Membranous septum defect most common (80%); L→R shunt → RV + pulmonary volume overload; Eisenmenger's = prolonged L→R → pulmonary hypertension → R→L reversal → cyanosis (late, irreversible) | Pansystolic murmur (LSE); spontaneous closure 50% by age 2 (muscular VSDs); patch repair for large/symptomatic |
| ASD (atrial septal defect) | ~10%; F>M | Ostium secundum (70%, fossa ovalis area); ostium primum (30%, near AV valves — associated with Down syndrome + AVSD); sinus venosus (near SVC + partial anomalous pulmonary venous drainage); L→R shunt → RV dilatation + right bundle branch block | Fixed split S2 (pathognomonic — atrial shunt prevents normal respiratory variation); catheter device closure (secundum); surgical for primum/sinus venosus |
| PDA (patent ductus arteriosus) | ~7%; common in prematurity | Ductus arteriosus = foetal communication between pulmonary trunk and descending aorta at left subclavian artery origin (T4 level); keeps open by PGE2 in foetus; normally closes within 24–48 h (O₂ + bradykinin); L→R shunt → pulmonary circulation overcirculation | Continuous "machinery" murmur (best heard below left clavicle); wide pulse pressure; treatment: indomethacin/ibuprofen (inhibit PGE2 synthesis) in neonates; surgical/catheter ligation if persistent |
1. Large VSD (subarterial/perimembranous — dextroposition of aorta means it overrides VSD)
2. Pulmonary outflow obstruction (infundibular stenosis ± valvular pulmonary stenosis)
3. Overriding aorta (aorta straddles the VSD, receiving blood from both ventricles)
4. Right ventricular hypertrophy (consequence of RVOTO)
Cyanosis: RVOTO causes RV pressure to equalise with LV → deoxygenated blood passes through VSD into overriding aorta → systemic desaturation. Degree of cyanosis depends on severity of RVOTO.
Tet spells (hypercyanotic episodes): acute infundibular spasm → ↑ RVOTO → ↑ R→L shunt → severe cyanosis → loss of consciousness. Management: knee-chest position (↑ SVR → ↓ R→L shunt), IV morphine (↓ infundibular spasm), IV propranolol (↓ spasm), IV fluids, O₂. CXR: "boot-shaped heart" (concave pulmonary segment + RV apex uplift). Total correction: patch VSD + relieve RVOTO; excellent long-term outcomes.
| Lesion | Anatomy | Key Feature |
|---|---|---|
| TGA (transposition of great arteries) | Aorta arises from morphological RV (anterior); pulmonary artery from morphological LV (posterior) — parallel circuits incompatible with life | Severe cyanosis from birth; survival = mixing (ASD/VSD/PDA); emergency Rashkind balloon atrial septostomy; definitive = Jatene arterial switch within first 2 weeks (re-implant coronary arteries) |
| Coarctation of aorta | Narrowing at juxtaductal position (at ligamentum arteriosum, distal to left subclavian); associated with bicuspid aortic valve (50%); Turner syndrome (45,XO) | Radio-femoral pulse delay; upper limb hypertension + lower limb hypotension; inferior rib notching on CXR (intercostal collaterals, appears after age 5–6); treat: balloon dilatation or surgical resection + end-to-end anastomosis in infancy |
Acyanotic → Cyanotic with Eisenmenger: "Left to Right until Pressure is Right" — L→R shunts (VSD/ASD/PDA) become cyanotic when pulmonary hypertension reverses them.
Cyanotic lesions (Right → Left from birth): 5 Ts — Truncus arteriosus, Transposition, Tricuspid atresia, Tetralogy of Fallot, Total anomalous pulmonary venous return (TAPVR).
Down syndrome cardiac lesions: AVSD (endocardial cushion defect = ostium primum ASD + inlet VSD) = most common; also VSD, ToF.
Turner syndrome: coarctation of aorta + bicuspid aortic valve.
- Most common CHD, its murmur, and spontaneous closure rate? VSD (30%); pansystolic murmur at left sternal edge; ~50% of muscular VSDs close spontaneously by age 2
- Fixed split S2 is pathognomonic of which lesion? ASD — atrial shunt equalises right and left filling throughout respiration, preventing normal respiratory variation in S2 splitting
- Four components of Tetralogy of Fallot (single embryological cause)? All from antero-superior deviation of infundibular septum: VSD + pulmonary outflow obstruction + overriding aorta + RV hypertrophy. CXR = "boot-shaped heart"
- Tet spell management? Knee-chest position (↑SVR → ↓ R→L shunt) + IV morphine (↓ infundibular spasm) + IV propranolol + IV fluids + O₂
- Coarctation of aorta: site, associations, and CXR finding? Juxtaductal narrowing at ligamentum arteriosum; associated with bicuspid aortic valve (50%) and Turner syndrome; CXR: inferior rib notching from intercostal collaterals (appears after age 5–6)
Fetal Circulation & Changes at Birth ★★★
The fetal circulation is built around one priority — getting the most oxygenated blood to the coronary arteries and brain — using three shunts: ductus venosus bypasses the liver, foramen ovale shunts oxygenated IVC blood directly to the LA, and ductus arteriosus dumps most RV output into the descending aorta away from the high-resistance fluid-filled lungs. A single event at birth — the first breath — simultaneously collapses pulmonary vascular resistance, reverses the foramen ovale pressure gradient (LA pressure now exceeds RA), and eliminates the PGE₂ source that was keeping the ductus arteriosus patent, sealing all three shunts within hours to weeks. The exam trap is vessel naming: the umbilical vein carries oxygenated blood (towards the fetus, from placenta) and the umbilical arteries carry deoxygenated blood (away from the fetus, to placenta) — opposite to all adult conventions.
The fetal circulation bypasses the non-functional lungs using three shunts: the ductus venosus, foramen ovale, and ductus arteriosus. Oxygenated blood from the placenta reaches the fetal heart via the umbilical vein, and deoxygenated blood is returned to the placenta via the umbilical arteries.
| Structure | Fetal function | Path | Adult remnant |
|---|---|---|---|
| Umbilical vein | Carries oxygenated blood from placenta to fetus (~80% O₂ saturation) | Umbilicus → liver → ductus venosus → IVC | Ligamentum teres hepatis (round ligament of liver) in falciform ligament |
| Ductus venosus | Bypasses hepatic circulation — shunts oxygenated blood from umbilical vein directly into IVC (bypasses liver sinusoids) | Portal vein → IVC junction | Ligamentum venosum (groove on posterior surface of liver) |
| Foramen ovale | Atrial-level shunt: shunts oxygenated blood from RA → LA (bypasses pulmonary circulation). Right atrial pressure > left atrial pressure in fetus (lungs not expanded) | IVC oxygenated blood preferentially streamed into RA → foramen ovale → LA → LV → aorta → coronary arteries + brain | Fossa ovalis (interatrial septum depression). Patent in 25–30% adults (PFO) — risk of paradoxical embolism → cryptogenic stroke |
| Ductus arteriosus | Arterial-level shunt: connects pulmonary trunk to descending aorta (just distal to left subclavian origin — T4 level). Bypasses pulmonary circulation. Shunts ~90% of RV output away from high-resistance fetal lungs | Pulmonary trunk → descending aorta | Ligamentum arteriosum. Patent in premature infants (PDA) — maintained open by PGE₂; closed by indomethacin (COX inhibitor) |
| Umbilical arteries (×2) | Carry deoxygenated blood from fetus back to placenta for re-oxygenation | Internal iliac arteries → umbilicus → placenta | Medial umbilical ligaments (lateral umbilical folds on inner anterior abdominal wall). Superior vesical arteries (proximal portion remains patent, supplies bladder) |
Ductus arteriosus: With first breath, PaO₂ rises → oxygen causes smooth muscle contraction of ductus wall → functional closure within 10–15 hours of birth; anatomical closure (ligamentum arteriosum) by 2–3 weeks. Prostaglandin E₂ (PGE₂) was keeping it open in utero — now declines as placental source is lost and lung metabolism destroys circulating PGE₂.
Ductus venosus: Umbilical cord clamping stops portal flow → ductus venosus closes functionally within minutes; fibroses within 2–3 weeks.
Umbilical vessels: Cord clamping → umbilical arteries constrict (muscular walls); umbilical vein closes. Both fibrosed within 3–7 days.
Net result: Series circulation established — pulmonary circuit (RV → lungs → LA) in series with systemic circuit (LV → body → RA). PVR drops from ~8× systemic at birth to adult levels by 6–8 weeks.
Ductus venosus → ligamentum venosum · Foramen ovale → fossa ovalis · Ductus arteriosus → ligamentum arteriosum · Umbilical vein → ligamentum teres hepatis · Umbilical arteries → medial umbilical ligaments.
Exam trap: The umbilical VEIN carries oxygenated blood (towards fetus); the umbilical ARTERIES carry deoxygenated blood (away from fetus — towards placenta). Opposite of adult convention.
- Three fetal shunts and their function? Ductus venosus (bypasses liver, umbilical vein → IVC); foramen ovale (RA → LA, bypasses pulmonary circulation); ductus arteriosus (pulmonary trunk → descending aorta, bypasses lungs)
- Adult remnants of fetal structures? Ductus venosus → ligamentum venosum; foramen ovale → fossa ovalis; ductus arteriosus → ligamentum arteriosum; umbilical vein → ligamentum teres hepatis; umbilical arteries → medial umbilical ligaments
- What closes the foramen ovale at birth and how? First breath → ↓ pulmonary vascular resistance → ↑ pulmonary venous return → ↑ LA pressure exceeds RA → flap valve closes functionally; anatomical fusion within weeks
- How does indomethacin close a PDA? Inhibits COX → ↓ PGE₂ synthesis; PGE₂ was keeping ductus smooth muscle relaxed (patent) in utero — removing it allows smooth muscle contraction and closure
- Which path does the most oxygenated blood take from placenta to fetal brain? Umbilical vein → ductus venosus → IVC → RA → foramen ovale → LA → LV → ascending aorta → carotids/brain (preferentially streamed by crista dividens)
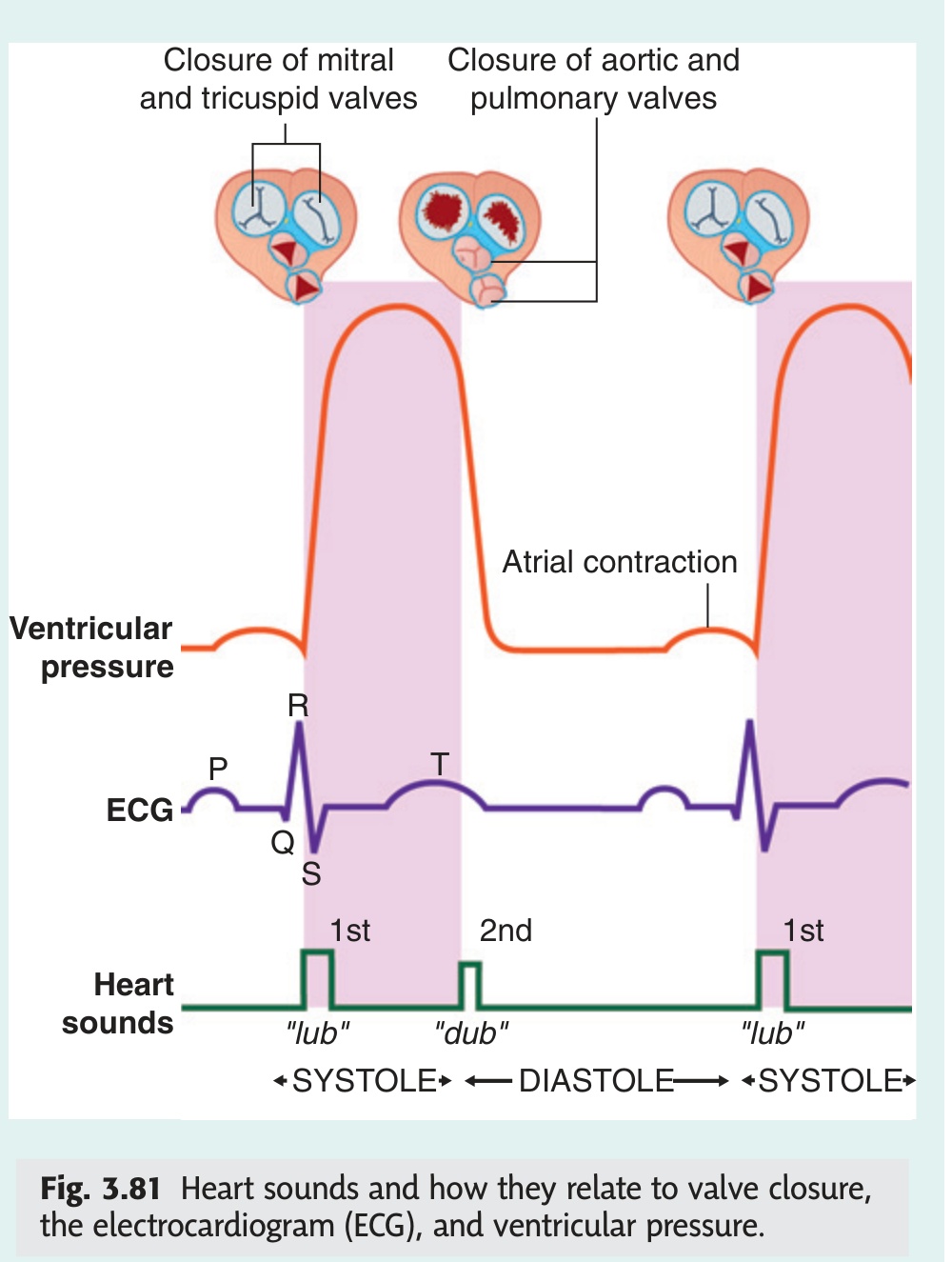
Heart Valve Murmurs — Quick Reference ★★★
Reading a murmur requires one orientation: S1 is AV valve closure (start of systole), S2 is semilunar valve closure (start of diastole). Systolic murmurs between S1 and S2 are either ejection murmurs (aortic/pulmonary stenosis — diamond-shaped, peaking mid-systole) or regurgitant murmurs (mitral/tricuspid regurgitation — flat pansystolic). Diastolic murmurs are always pathological: an early high-pitched decrescendo immediately after S2 signals aortic regurgitation (blood falling back through an incompetent aortic valve), while a rumbling low-pitched mid-diastolic murmur after an opening snap signals mitral stenosis. Murmur radiation follows blood flow: aortic stenosis to the carotids, mitral regurgitation to the axilla.
A murmur is turbulent blood flow across a valve. Stenosis = obstructed forward flow (turbulence downstream). Regurgitation = backflow through an incompetent valve (turbulence in wrong direction). Timing relative to S1 and S2 is the primary diagnostic tool.
| Lesion | Timing | Quality | Best Heard | Radiation | Key Feature |
|---|---|---|---|---|---|
| Mitral stenosis | Mid-diastolic (after opening snap) | Low-pitched rumble | Apex; left lateral decubitus | None | Opening snap precedes murmur; OS closer to S2 = more severe; louder in expiration |
| Mitral regurgitation | Pansystolic (S1 → S2) | High-pitched blowing | Apex; left lateral decubitus | Left axilla + left infrascapular | Masks S1; widely split S2; louder in expiration; hyperdynamic apex beat |
| Aortic stenosis | Ejection systolic (crescendo–decrescendo) | Harsh, rasping | 2nd right ICS (aortic area) | Both carotid arteries | Slow-rising (pulsus parvus et tardus) carotid; narrow pulse pressure; paradoxical S2 split; SAD triad (Syncope → Angina → Dyspnoea) |
| Aortic regurgitation | Early diastolic (decrescendo) | High-pitched blowing | 3rd–4th left ICS (left sternal edge); sitting forward, expiration | None | Collapsing (water-hammer) pulse; wide pulse pressure; de Musset's sign (head bobbing); Austin Flint murmur (functional MS at apex) |
| Tricuspid stenosis | Mid-diastolic | Low-pitched rumble | Lower left sternal border (4th ICS) | None | Increases with inspiration (Rivero-Carvalho sign); elevated JVP with prominent a-wave; rare — usually rheumatic |
| Tricuspid regurgitation | Pansystolic | Soft blowing | Lower left sternal border | None | Increases with inspiration (Carvallo's sign); pulsatile liver; prominent cv-wave in JVP; often functional (RV dilation) |
| Pulmonary stenosis | Ejection systolic | Harsh | 2nd left ICS (pulmonary area) | Left shoulder | Widely split S2 (delayed P2); RV heave; ejection click (valvular PS); seen in ToF; increases with inspiration |
| Pulmonary regurgitation | Early diastolic | High-pitched blowing | 2nd–3rd left ICS | None | Graham Steell murmur = PR due to pulmonary hypertension (e.g. mitral stenosis); increases with inspiration |
RILE rule — Inspiration vs Expiration:
Right-sided murmurs increase with Inspiration (↑ venous return to right heart)
Left-sided murmurs increase with Expiration (or left lateral decubitus)
PASS — Systolic murmur causes: Pulmonary stenosis · Aortic stenosis · MR · TR (pansystolic = MR, TR, VSD)
SAD triad for aortic stenosis prognosis (mean survival without intervention):
Syncope → 3 years · Angina → 5 years · Dyspnoea → <2 years
Mitral murmurs (stenosis + regurgitation): always auscultate in left lateral decubitus with the bell of the stethoscope at the apex — this brings the LV apex closer to the chest wall.
Aortic regurgitation: patient sits forward, holds breath in full expiration — brings the aortic root closer to the anterior chest wall; use the diaphragm at the left sternal edge.
Inspiration manoeuvre (Rivero-Carvalho / Carvallo's sign): tricuspid murmurs increase because inspiration ↓ intrathoracic pressure → ↑ venous return → ↑ right heart filling → louder right-sided murmur.
Valsalva manoeuvre: ↓ venous return → most murmurs softer — EXCEPT hypertrophic obstructive cardiomyopathy (HOCM) and MVP prolapse murmurs, which become louder (decreased LV volume worsens obstruction/prolapse). [Gray's 4e Ch3 p179]
| Chamber | Inlets | Outlet | Key Internal Feature | Exam Note |
|---|---|---|---|---|
| Right Atrium | SVC orifice IVC orifice Coronary sinus orifice |
Right AV orifice (tricuspid valve) | Fossa ovalis; crista terminalis; pectinate muscles | 3 inlets = most tested |
| Right Ventricle | Right AV orifice (tricuspid) | Pulmonary orifice (pulmonary valve) | Septomarginal trabecula (moderator band); conus arteriosus | Moderator band = right bundle branch |
| Left Atrium | 4 pulmonary vein orifices | Left AV orifice (bicuspid/mitral valve) | Smooth posterior wall; left auricle | 4 pulmonary veins = always tested |
| Left Ventricle | Left AV orifice (bicuspid/mitral) | Aortic orifice (aortic valve) | Thickest wall; aortic vestibule; aortic sinuses → coronary arteries | Thickest wall = 3× right ventricle |
- S1 and S2 — what causes each? S1 = closure of AV valves (mitral + tricuspid) at start of systole. S2 = closure of semilunar valves (aortic + pulmonary) at start of diastole
- Aortic stenosis murmur: timing, quality, radiation, pulse character? Ejection systolic (crescendo-decrescendo); harsh; radiates to carotids; slow-rising pulsus parvus et tardus; narrow pulse pressure; paradoxical split S2
- Mitral regurgitation murmur: timing and radiation? Pansystolic (flat); high-pitched; loudest at apex; radiates to axilla; associated with a soft S1
- Aortic regurgitation murmur: timing and associated signs? Early diastolic decrescendo immediately after S2; high-pitched; best heard at lower left sternal edge leaning forward; wide pulse pressure; collapsing (waterhammer) pulse; Corrigan's sign
- Mitral stenosis murmur: timing and special feature? Rumbling mid-diastolic (after opening snap); low-pitched; best heard at apex with bell in left lateral decubitus; loud S1; opening snap (OS) — shorter S2-OS interval = more severe stenosis